These are not common. However they tend to occur in children and young adults. They arise from minor salivary glands in the lower lip and the floor of the mouth. The reason is that unlike the parotid or submandibular gland, the minor salivary glands can secrete against pressure. If a duct is torn then saliva will be pumped out of the leak into the surrounding soft tissues and collect as a fluid filled sac.
Mucocele
These form mainly in the lower lip and are caused by chewing or damaging one of the many minor salivary glands that fill the lip. A blueish balloon then forms which occasionally pops then refills.
Our Treatment
Treatment is a simple operation to excise the cyst and is performed under local anaesthesia in an outpatient setting.
Mucocele
Simple Ranula
Simple Ranula
The collection of minor salivary glands in the floor of the mouth is called the sublingual gland. If one of these minor ducts is damaged then the same process starts as described for mucocele. But as there is more space in the floor of the mouth, these sacs can grow to a large size.
A wide variety of treatments have been described for simple ranulae but all are unreliable. The treatment normally offered is still the removal of the sublingual gland. This is a tricky operation, usually unnecessary and painful.
Our Treatment
We have developed a simple and effective technique (85% success) for simple ranulae shown in Prof McGurk’s video opposite. We drain the cyst using a fine needle, the patient is reviewed the next day at which time the sac is starting to fill with saliva again. This small collection of fluid accurately locates the site of the leaking duct. A surgical stitch (suture) is inserted to strangle the leak. This procedure is easily tolerated by most children and is carried out under local anaesthetic.
Our development has been very welcome since many ranulae occur in children and the traditional alternatives are often painful.
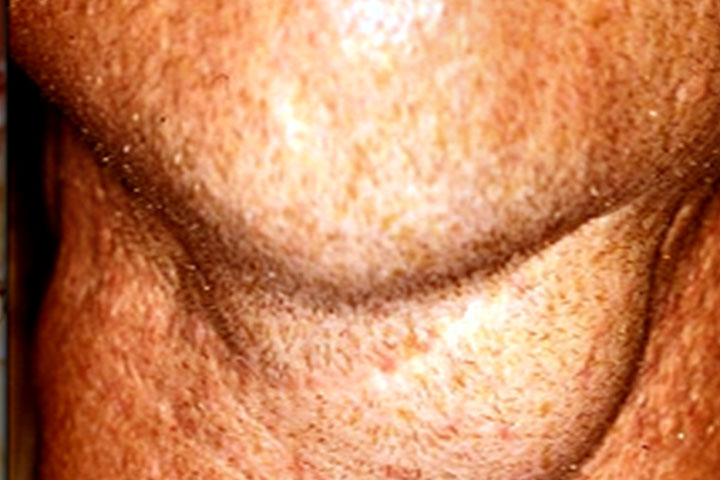
Plunging Ranula
This is the least common form of ranula. In this instance the leak of saliva comes from the under surface of the sublingual gland and collects on the surface of the muscle that forms the floor of the mouth. Eventually the fluid finds a way through the muscle fibres to collect in the neck under the lower border of the mandible to lie next to the submandibular gland.
Historically the leak of saliva was thought to come from the submandibular gland, this led surgeons to erroneously remove the this gland instead of the sublingual gland.
The traditional treatment, still common in the UK, is to remove both the submandibular gland as well as the sublingual gland.
It is no longer necessary to remove both glands.
Careful diagnosis is important because it can be confused with a different condition called a lymphangioma. It is important to distinguish between the two as they are treated differently.
Our Treatment
At surgery, the sublingual gland is freed from the floor of mouth and pulled upwards. The neck of the sac which is attached to the sublingual gland is drawn into the mouth. The sac is emptied of saliva, it’s neck tied and it is allowed to descend back below the muscle into the neck where it dissolves. This approach avoids a second incision in the neck.